AUCTORES
Globalize your Research

Case Report | DOI: https://doi.org/10.31579/2578-8949/038
*Corresponding Author: Ethan Nicholas, Department of Dermatology, Provençals 33, Barcelona, Spain.
Citation: Ethan Nicholas, Benjamin Dylan, and Dominic Chase. Sex Hormones Production in Both Genders Skin Diseases. J .Dermatology and dermatitis. Doi:10.31579/2578-8949/038
Copyright: © 2018 Ethan Nicholas. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 08 June 2018 | Accepted: 30 June 2018 | Published: 06 July 2018
Keywords: gender; skin; dermatoses; sex hormones
The skin is the largest organ in the body constituting 15% of the total body weight. It is therefore paramount to address skin diseases. Of major importance in the etiopathogenesis and pathophysiology of many of these diseases is the gender difference in the skin. Studies on endocrine effects on the skin have revealed that several important physiologic activities of the skin are either partly or wholly under the control of hormones secreted by different endocrine glands.
The skin is an endocrine organ involved in the peripheral conversion of sex hormones to active forms (testosterone and DHT in males and estradiol in females). Skin structures such as sebocytes, sweat glands and dermal papilla hair cells express enzymes that convert DHEA and androstenedione from adrenal cortex into testosterone and DHT. Aromatases convert testosterone into estradiol in the skin. The sebaceous glands, the outer and inner root sheath cells of anagen terminal hair follicles and dermal papilla cells express aromatases. Various structures in the skin show enzyme activity and express sex hormone receptors [1]. Epidermal keratinocytes contains androgen receptors (AR), estrogen receptor-beta (ERβ), and the enzymes 17β hydroxysteroid dehydrogenase (HSD) and 5α-reductase. Melanocytes express the AR, ERα and ERβ receptors. A disease is an aberration in the normal. This could be in the form of changes in structure or function. The functions of the skin have to be considered in relation to its structure i.e. the structure definitely determines its function. Structural and physiological changes in the skin can occur as a result of infection, genetic changes, physical factors (such as heat), nutritional diseases, metabolic derangements, cosmetic use, drug use, organ malfunctions, environmental factors (specific for the individual, for example, occupation, social lifestyle, geographical location, antibiotics use, the use of cosmetics and soaps), and endocrine changes.
The study of skin diseases is often related to age groups and environmental factors while their relationship to gender has not been fully elucidated. Differences in the structures and functions of the skin in both genders underline the gender differences observed in many skin diseases. Various structures in the skin are under the influence of endocrine activities in the skin or outside the skin. Sex hormones – androgens and estrogens – influence the skin structure and functions.
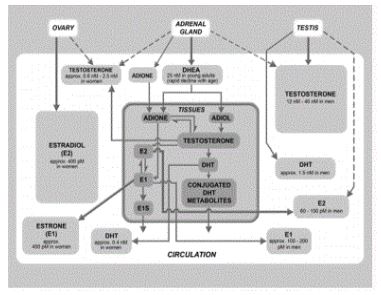
In young men, testes produce testosterone and in young women, ovaries are the main source of estradiol (Figure 1) [1]. Sex steroids are produced by the hypothalamic-pituitary-gonadal axis, the adrenals (which produce dehydroepiandrosterone (DHEA) and androstenedione – precursors of androgens and estrogens in peripheral tissues), and by peripheral tissues (Figure 2) [1].
With aging, gender differences occur in serum concentrations of these hormones. In men, gonadal production of androgens slowly decreases and by 65 years, peripheral tissues such as skin produce 40% of the total androgens [2]. In women, the peripheral tissues produce almost all the sex steroids from DHEA after menopause [3]. In both genders, a gradual decline in DHEAS and DHEA occurs with age and this is thought to contribute to the degenerative changes seen with aging [4-8].
The effect of sex hormones differs in men and women [9]. Androgens affect several functions of the human skin, such as sebaceous gland growth and differentiation, hair growth, epidermal barrier homeostasis and wound healing [10]. Facial, axillary and pubic hairs respond to androgens while the eyebrows and eyelashes do not. Hence, masculinizing syndromes in women are usually accompanied by hirsutism [11]. Removal of testicular hormones in men results in reduction of beard growth, and re-growth of beard occurs when treated with androgens [12]. Excess testosterone in females results in androgenetic-dependent alopecia while excess testosterone (by increasing sebum production) in males predisposes to severe acne and removal of testosterone results in reversal of male-pattern hair loss [1,13,14].
Wound healing is slower in males. Trauma results in changes in sex steroid concentrations with higher estrogen concentrations in both sexes and decreased testosterone levels in males [15-18]. At physiological levels, 5-α-dihydrotestosterone (5α-DHT) decrease wound immune function and impair wound healing after trauma and hemorrhage by increasing proinflammatory cytokines and decreased tumor growth factor-β at the wound site [19,20]. The male skin is thicker than female skin [21]. Females, however, have thicker subcutaneous tissues [22]. Female skin becomes thinner than male skin with aging due to reduction in estrogen [23,24]. Estrogen therapy increases skin thickness [25].
Skin surface pH, and sweat rate are higher in males [9]. With the higher skin surface pH, the resultant effect is that microbial diversity is often lower in men as they are hindered by more acidic environments [26]. Trans-epidermal water loss (TEWL), erythema index and melanin index were found to be higher in men living in hot areas while women have higher skin hydration and elasticity [27]. Young men have higher SC hydration in comparison with women until the age of 40 when it progressively decreases while it remains stable or even increase in women with age [28].
Sex steroids have a differential effect on the immune system in men and women. Androgens are anti-inflammatory and depress both cellular and humoral immunity resulting in men having higher susceptibility to skin infections [29-31]. Men are more prone to bacterial and viral infections though they have less microbial diversity in their skin than women due to more acidic skin pH [9,26].Estrogens stimulate the humoral immunity and causes development of auto reactive B cells, and inhibit apoptosis which results in survival of auto reactive T cells. Autoimmune diseases such as SLE and allergic contact dermatitis (related to occupation) occur more in women as a result of these effects [15].

Research studies involving skin physiology are very few in Nigeria. Not many studies have been performed to determine the relationship between gender and skin diseases. In a study by Oninla et al. [30] at Ile-Ife, gender predilection was studied among 1,013 patients presenting with 1,097 dermatoses [30]. A comparison was made with a study reporting the prevalence of skin diseases in both genders. Viral warts, follicullitis/carbunculosis, Hansen’s disease, elephantiasis were found to have a significant relationship with the male gender [31]. As mentioned earlier, bacterial and viral infections are more common in males. Infections seen more in females but not significant in them were can did an intertrigo, herpes zoster and onchodermatitis.
Few studies have been done in Nigeria on the effect of gender on skin diseases. Studies of dermatological conditions in relation to measured hormone levels as well as skin physiological changes by hormones in both genders are needed.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.





























































